Of all the industries subject to government management, healthcare is perhaps the most emotionally charged. Access to medical care is widely viewed as a fundamental human right, a necessity that lies beyond the standard laws of economics. When a person is sick or injured, they cannot shop around for prices or decline service the way they can with consumer electronics or travel. Because of this inherent vulnerability, the consensus among policymakers across the political spectrum is that the healthcare market is unique, requiring extensive regulation, subsidies, price controls, or outright state ownership to function in a compassionate society.
This consensus gets the relationship backwards. The unique problems of modern healthcare: soaring prices, administrative bloat, supply shortages, and rationing by delay: are not failures of the market. They are the predictable consequences of state intervention. By decoupling the consumer from the price, restricting the supply of doctors and facilities, and cartelizing the insurance and pharmaceutical markets, the government has perverted the economics of medicine. Analyzing how these interventions operate, examining how they manifest in different systems across twenty nations, and proposing a path toward free-market reform is essential to understanding how we can build a system that is both economically sustainable and genuinely compassionate.
The Libertarian Critique: The Perverted Economics of Medicine
To understand the failure of modern healthcare systems, one must apply the basic principles of economics to the medical market. The market is not a machine; it is a network of human cooperation coordinated by price signals. When these signals are distorted, the coordination breaks down.
In a normal market, consumers pay directly for goods and services. Because they are spending their own money, they are highly sensitive to both price and quality. They seek out the best value, forcing providers to compete by lowering costs and improving service. This competition drives efficiency and makes goods affordable to the wider public.
Modern healthcare has replaced this system with a third-party payer model. Whether through private insurance or government programs, the vast majority of medical transactions are paid for by an entity other than the patient. This creates a severe moral hazard. Because patients pay only a tiny fraction of the actual cost at the point of service, they have no incentive to be cost-conscious. They demand unlimited treatments, tests, and specialists, regardless of cost.
Providers respond to these incentives. Because they are billing an insurance company or a government agency rather than the patient, they do not compete on price. Instead, they compete on administrative compliance and technology, raising their prices to capture the maximum possible reimbursement from the third-party payer. The link between consumer choice and price is severed, leading to a perpetual spiral of rising expenditures.
Furthermore, the state uses its regulatory power to restrict the supply of medical services. Through occupational licensing, building restrictions, and drug approval barriers, the government keeps the supply of care artificially low while subsidies keep demand high. The combination of stimulated demand and restricted supply can only result in one outcome: soaring prices and rationing.
The Distorted Reality of the United States Healthcare System
The United States healthcare system is frequently criticized by defenders of state medicine as an example of a failed free market. This claim is historically and economically illiterate. The US system is not a free market; it is a heavily regulated, corporatist cartel shaped by decades of federal intervention.
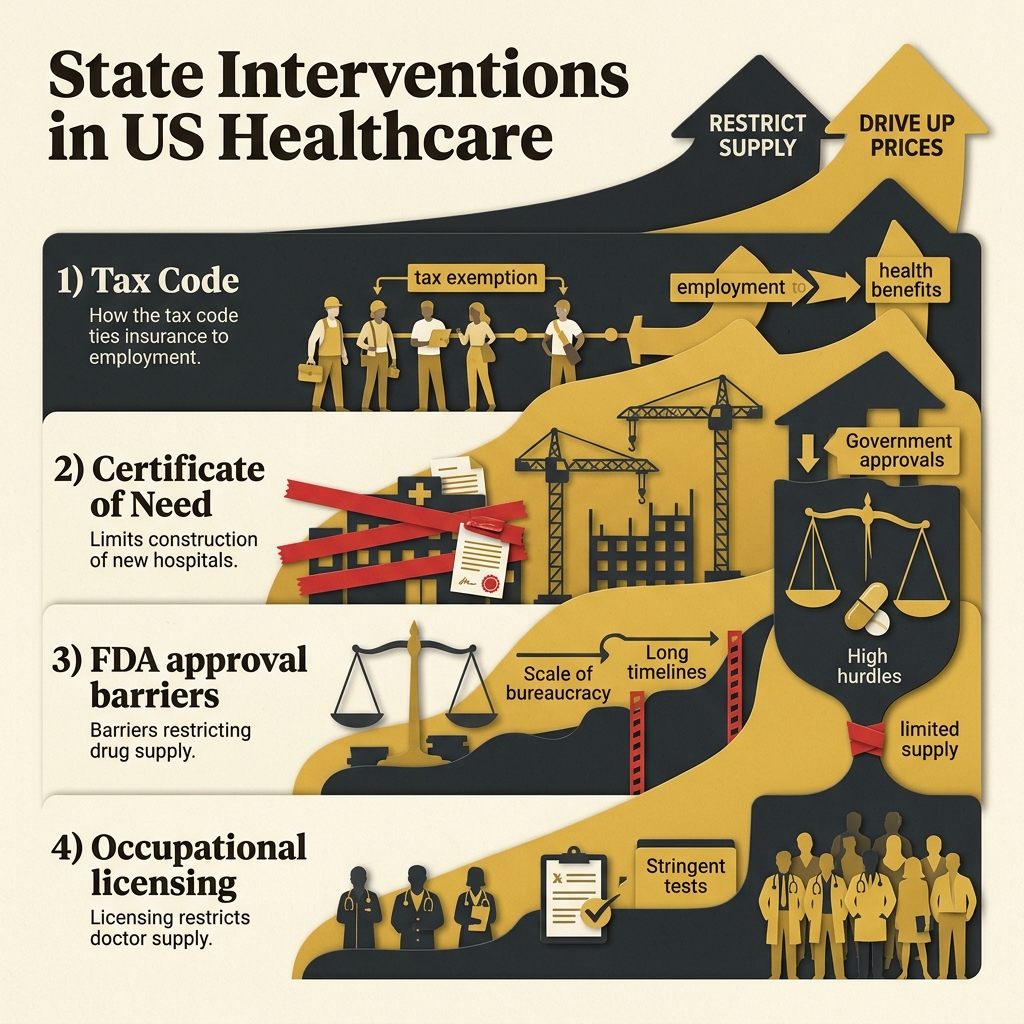
The distortions of the US system can be traced to several key interventions.
The Employer-Provided Insurance Tax Exemption
The reason the United States relies on employer-provided health insurance, a system that creates widespread job lock and inefficiency, is a historical tax distortion. During World War II, the federal government imposed wage controls to curb inflation. To attract workers without violating these controls, businesses began offering health benefits.
In 1943 and later codified in 1954, the Internal Revenue Service ruled that employer contributions to health insurance were tax-exempt, while individual purchases of insurance were not. This policy created a massive tax subsidy for employer-provided plans.
This tax distortion transformed health insurance from a safety net for catastrophic events (like car accidents or cancer) into a pre-paid medical maintenance scheme. Imagine if automobile insurance covered oil changes, gasoline, and windshield wiper replacements; the cost of auto insurance would soar, price transparency would disappear, and mechanics would spend their days billing insurance companies rather than serving customers. This is exactly what happened to US medicine.
Certificate of Need (CON) Laws
In 1974, the federal government mandated that states implement Certificate of Need (CON) laws. These laws require healthcare providers to obtain permission from a state board before building new hospitals, expanding existing facilities, purchasing expensive medical equipment, or offering new services.
The stated goal was to prevent over-investment and lower costs. The actual result was regulatory capture. The state boards are typically dominated by representatives from existing, incumbent hospitals. These incumbents use their power to deny certificates to new competitors, protecting their monopolies and keeping the supply of local hospital beds and diagnostic machines artificially low. Although the federal mandate was repealed in 1986, dozens of states retain CON laws, restricting access to care and driving up hospital prices.
The FDA Supply Monopoly
The Food and Drug Administration (FDA) holds a complete monopoly on the approval of pharmaceuticals, medical devices, and diagnostic tests in the United States. While safety and efficacy are the stated goals, the FDA approval process is a massive regulatory barrier.
It takes an average of ten to twelve years and over one billion dollars to bring a new drug to the US market. These immense hurdles favor large, politically connected pharmaceutical giants (Big Pharma) while driving smaller startups out of business. Furthermore, the FDA prohibits the importation of safe, identical pharmaceuticals from other developed countries (such as Switzerland or Japan) that have approved them through their own rigorous processes, shielding domestic pharmaceutical companies from foreign competition and keeping drug prices in the United States higher than anywhere else in the world.
Occupational Licensing and residency limits
The supply of medical professionals in the United States is strictly limited by the state, largely through the lobbying influence of the American Medical Association (AMA). In the early twentieth century, the AMA successfully lobbied to shut down medical schools that did not meet its centralized standards, significantly reducing the number of doctors graduated per year.
Today, the supply of new doctors is restricted by federal caps on funding for residency programs, which have not kept pace with population growth. The government also uses licensing laws to restrict the scope of practice for nurse practitioners, physician assistants, and midwives, prohibiting them from diagnosing routine illnesses or prescribing basic medicines without the supervision of an expensive licensed physician. This artificial doctor shortage inflates wages for specialists while reducing the availability of primary care for patients.
Comparative Global Analysis: 20 Countries Under the Microscope
To evaluate the effects of government management on medicine, we must examine the healthcare structures of other countries. By analyzing the incentives, wait times, rationing mechanisms, and outcomes of twenty national systems, we can identify what works and what fails from an economic perspective.
1. United Kingdom: The Beveridge Archetype
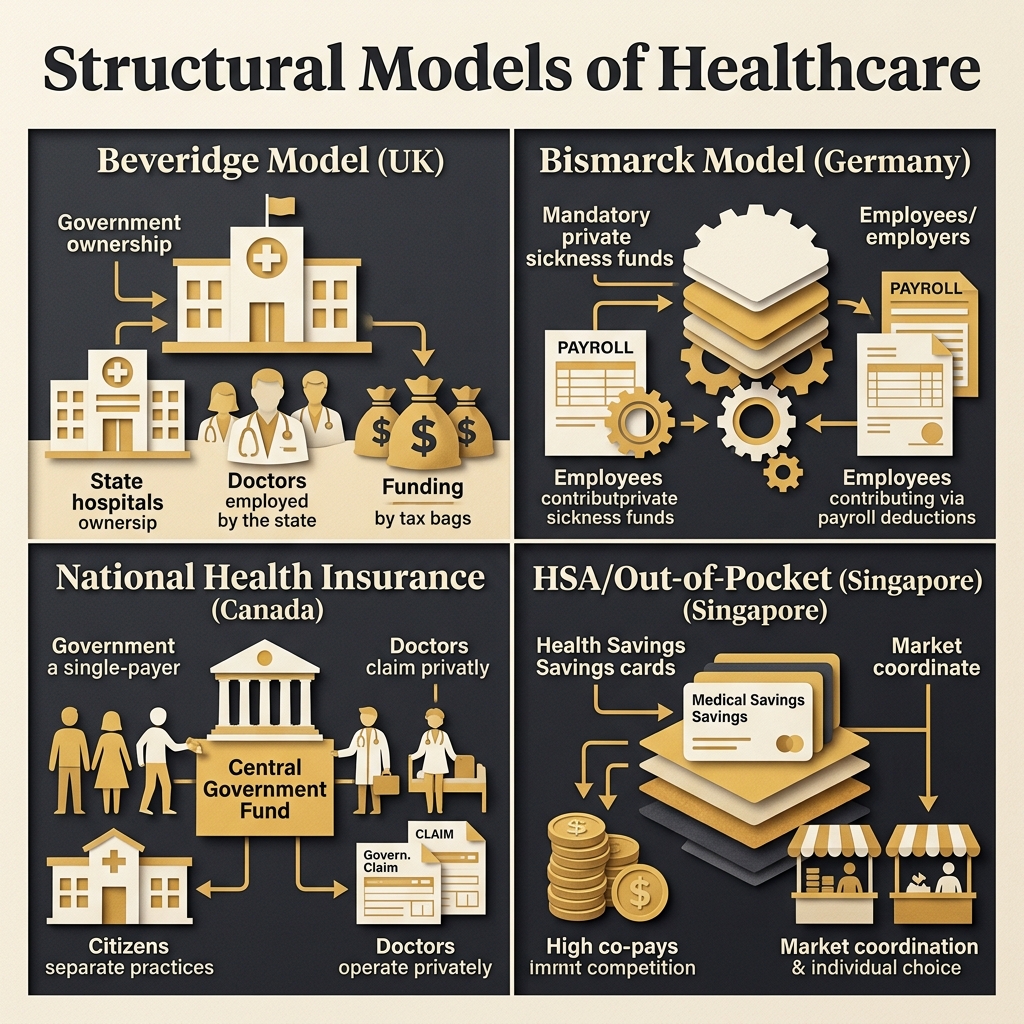
The British National Health Service (NHS) is the purest example of the Beveridge model. The government owns the hospitals, employs the doctors and nurses, and funds the entire system through progressive taxation. Care is free at the point of service.
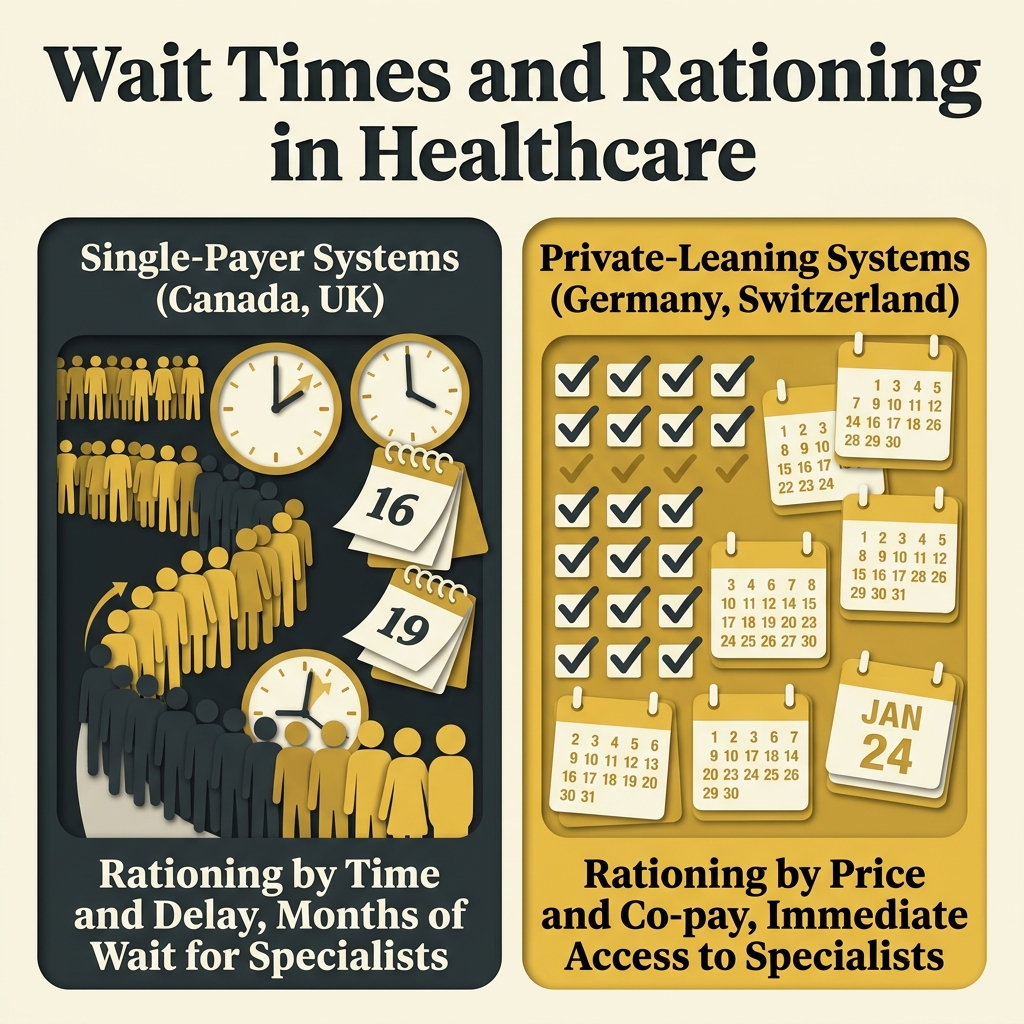
Because price is set to zero, the demand for NHS services is near-infinite. Since resources are limited, the NHS must ration care by time. The result is chronic, systemic wait times for elective surgeries, cancer treatments, and specialist appointments, with hundreds of thousands of patients waiting over a year for routine procedures. Doctors and nurses are underpaid compared to their international peers, leading to frequent strikes and a brain drain of talent to private systems abroad. To bypass these delays, a growing percentage of the British population purchases supplementary private insurance, creating a de facto two-tiered system despite the political commitment to universal equality.
2. Canada: The Single-Payer Monopoly
Canada operates a single-payer system (often called Medicare) where the government acts as the sole insurer, while the majority of doctors and hospitals operate in the private sector but bill the provincial governments according to a fixed fee schedule.
To maintain budget control, Canadian provincial governments impose strict global caps on hospital budgets and limit the number of approved specialists and diagnostic machines. Because private, competing insurance for core medical services was historically banned in most provinces, patients have no legal way to purchase care domestically to escape wait lists. This has led to severe queues, with the average wait from GP referral to specialist treatment exceeding twenty-five weeks. Tens of thousands of Canadians travel to the United States or other foreign countries every year to purchase surgeries out-of-pocket, demonstrating that Canada's universal system relies on the private capacity of other nations to act as a safety valve.
3. Germany: The Bismarck Pioneer
Germany's system is based on the Bismarck model. Insurance is mandatory and provided through a network of non-profit, competing private insurance funds (sickness funds) funded by payroll taxes split between employers and employees.
Germany allows citizens earning above a specific income threshold to opt out of the public sickness funds entirely and purchase private health insurance. This private option injects competition and cash into the system, allowing private insurers to pay doctors higher fees, which subsidizes the infrastructure of the entire market. Wait times are significantly shorter than in the UK or Canada. However, Germany faces soaring costs due to demographic aging and a lack of price discipline, as the payroll tax rates required to fund the sickness funds must continuously rise, dragging down economic competitiveness.
4. France: High Subsidies and Supplementary Mutuals
France runs a national health insurance system funded by payroll taxes and general income taxes. The state insurer covers seventy to eighty percent of medical costs, and citizens typically purchase supplementary, non-profit mutual insurance plans to cover the remainder.
France offers high patient choice, allowing citizens to see any doctor or specialist they choose without gatekeeping. However, this lack of restriction leads to high utilization and massive deficits for the state insurance fund. The government continuously tries to rein in costs by lowering reimbursement rates for medicines and increasing out-of-pocket co-pays, transferring the burden back to consumers and their supplementary mutuals.
5. Switzerland: Mandatory Private Competition
Switzerland rejected state-run medicine in favor of a universal private model. All residents are required to purchase basic health insurance from competing private insurers. The government subsidizes premiums for low-income citizens, but there are no state-run public options.
To encourage cost-consciousness, Swiss plans require deductibles and a ten percent co-insurance payment up to a specific cap. The system delivers high quality, short wait times, and rapid innovation, as insurers compete for customers. However, because the government mandates a highly comprehensive basic benefits package that every plan must cover, insurers cannot offer low-cost, minimal-coverage plans. This mandate keeps premium costs high, making Swiss healthcare among the most expensive in the world on a per capita basis.
6. Singapore: The HSA-Centric Model
Singapore operates one of the most economically efficient healthcare systems in the world, combining individual responsibility with a targeted public safety net. The system is built around the 3M framework: Medisave, Medishield Life, and Medifund.
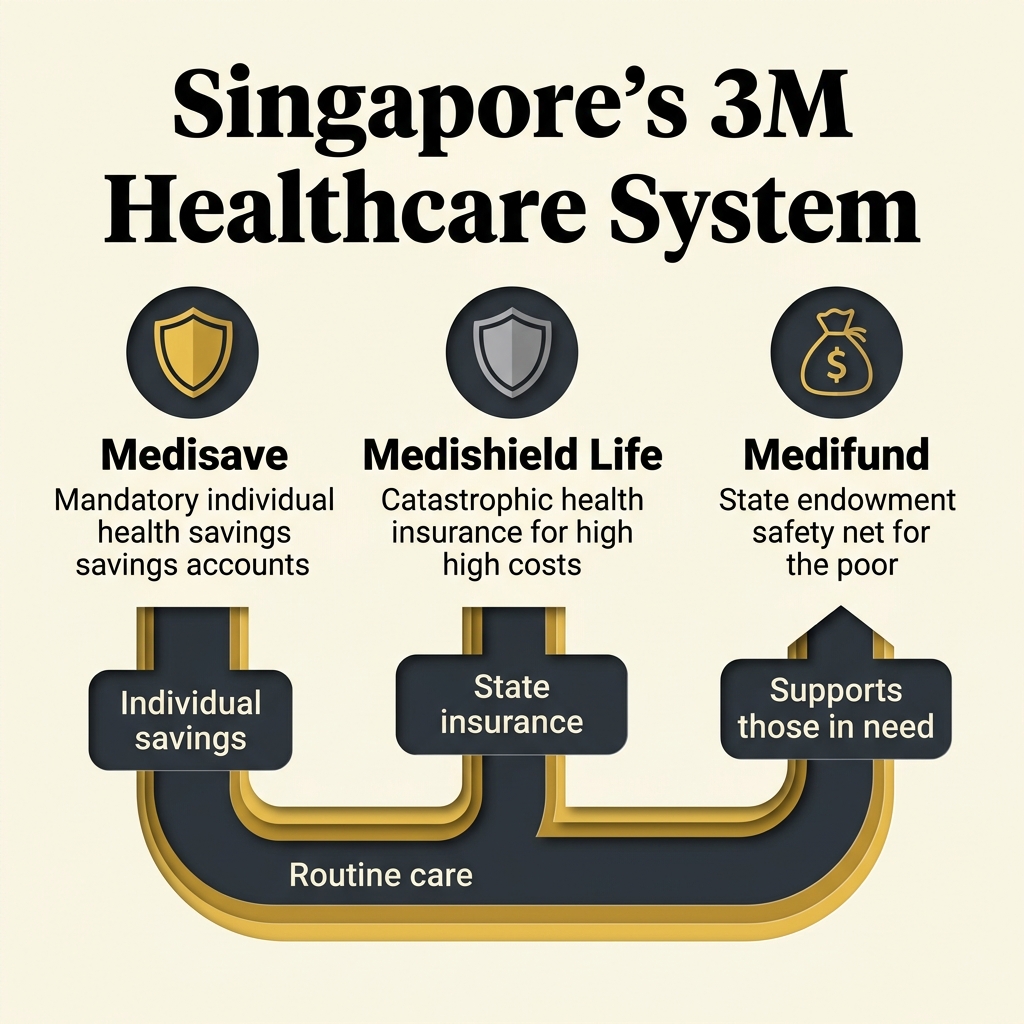
Medisave is a mandatory health savings account where workers save a portion of their income to pay for routine medical expenses. Because patients spend their own Medisave funds, they are highly price-sensitive, forcing providers to compete on price and publish cash prices transparently. Medishield Life is a catastrophic, state-managed insurance plan that covers high costs for surgeries and chronic illnesses. Medifund is a government-funded endowment safety net that pays the bills of the poorest citizens. While Singapore delivers excellent health outcomes at a fraction of the cost of Western nations, the system is not entirely free-market; the government tightly regulates the supply of hospital beds, controls the training slots for doctors, and sets price ranges for public ward classes.
7. Australia: The Dual Public-Private Track
Australia operates a dual system consisting of a universal public single-payer (Medicare) funded by an income tax surcharge, running alongside a heavily subsidized private insurance sector.
To relieve pressure on the public system, the Australian government penalizes high-income earners who do not purchase private health insurance by charging them an additional tax levy (the Medicare Levy Surcharge). It also provides tax rebates for private premium payments. This policy keeps nearly half the population in private insurance, ensuring short wait times for private patients while keeping public queues manageable. However, the subsidies represent a massive fiscal transfer from taxpayers to private insurance companies, distorting market prices.
8. Japan: Fee Schedules and High Utilization
Japan operates a statutory health insurance system where all citizens are covered through employer-based plans or national community plans. Doctors and hospitals operate privately, but the government sets a strict national fee schedule that dictates the price of every procedure and medicine.
Japan has no gatekeeping, allowing patients to see specialists at any time, leading to very high utilization: the average Japanese citizen visits the doctor over twelve times a year, compared to four times in the United States. Because the fee schedule keeps prices artificially low, hospitals must make up for low margins through volume, leading to short consult times and long hospital stays where patients are kept in beds longer to maximize revenue. The system faces a severe funding crisis as the aging population requires more care than the fixed fee schedule can sustain without massive subsidy injections from the national budget.
9. Sweden: Decentralized Regional Beveridge
Sweden's healthcare is organized under a decentralized Beveridge model. The country is split into regions, and each region's council levies local taxes to fund and manage local hospitals and clinics.
Decentralization allows regions to tailor services to local populations, but it also creates massive inequalities in access and wait times across the country. Sweden struggles with long queues for specialist care, particularly in child psychiatry and oncology, leading the government to introduce a national guarantee (the 90-day rule) that promises care within three months. Like most state guarantees, this is frequently bypassed in practice through administrative classification, as regions struggle to recruit sufficient doctors and nurses under fixed public salary scales.
10. Netherlands: Managed Private Competition
The Netherlands overhauled its healthcare system in 2006, replacing a multi-tiered public-private split with a single, universal private insurance market. All citizens must purchase a basic package from competing private insurers, who must accept all applicants regardless of pre-existing conditions.
To prevent selection bias, the government operates a sophisticated risk equalization pool that compensates insurers who take on high-risk, sick patients. While the system delivers high quality and has eliminated wait times, it has led to consolidation in the insurance sector: four large insurance conglomerates now control ninety percent of the market. These giants act as powerful cartel managers, setting terms for hospitals and doctors, reducing consumer choice, and keeping premium costs rising steadily.
11. Taiwan: The Smart Card Single-Payer
Taiwan established its National Health Insurance (NHI) system in 1995, consolidating multiple insurance funds into a single, government-run insurer. All citizens carry an NHI smart card that contains their full medical history and is swiped at every visit to track treatments and prevent abuse.
Taiwan's system is highly convenient and has very low administrative costs (under two percent). However, because patients can see any specialist without a referral for small co-payments, hospitals are overcrowded and doctors are severely overworked, facing burnout and low pay under the government's strict global budget caps. The NHI is perpetually on the brink of insolvency, as politicians refuse to raise premium rates on voters, leading to under-investment in new, expensive medical technologies and long-term sustainability issues.
12. South Korea: High-Volume Supply Squeeze
South Korea operates a single-payer system managed by the National Health Insurance Service. Healthcare providers are overwhelmingly private, but must accept the government's fixed reimbursement rates.
The system offers rapid, high-tech diagnostic services, but suffers from severe supply-side imbalances. Because the government sets low prices for primary care and pediatrics while allowing higher margins for plastic surgery and cosmetic procedures, new doctors are fleeing essential medicine. Major hospitals face pediatric physician shortages, and patients frequently wait hours in emergency rooms, demonstrating how price controls distort the career choices of medical professionals and create artificial shortages in critical care areas.
13. Norway: Oil-Funded Public System
Norway operates a universal public healthcare system funded by national and municipal taxes, heavily subsidized by the country's sovereign oil wealth.
The oil-fund cushion allows Norway to spend vast sums on state-of-the-art hospital infrastructure and maintain high nurse-to-patient ratios. However, even with near-unlimited funding, the Norwegian system still suffers from rationing by delay, with wait lists for psychiatric services and orthopedic surgeries. This demonstrates that when price signals are removed, even the wealthiest nations cannot spend their way out of the supply shortages caused by central planning.
14. Denmark: Municipal Gatekeeping
Denmark's system is funded by a national tax and managed by five regional councils that run public hospitals. GPs act as strict gatekeepers, receiving capitation fees to manage primary care and controlling referrals to specialists and hospitals.
Gatekeeping keeps hospital costs low, but it creates a frustrating barrier for patients, who must convince their GP to grant them access to specialist treatment. The system is highly digitized, which reduces administrative errors, but suffers from nursing shortages and long wait lists for cancer follow-ups, leading to political battles over regional funding allocations.
15. New Zealand: Public System with Growing Private Safety Valve
New Zealand operates a public healthcare system funded by general taxation, with District Health Boards managing local care.
The public system faces severe budget constraints, leading to strict rationing of elective surgeries: patients are placed on active care lists only if their condition is classified as severe enough. To escape this rationing, more than one-third of the population purchases private health insurance, allowing them to access private hospitals and clinics that operate alongside the public sector. The public system effectively relies on this private safety valve to manage capacity.
16. Israel: Non-Profit HMO Sickness Funds
Israel requires all citizens to register with one of four competing, non-profit sickness funds (HMOs) funded by a payroll tax. The government distributes these funds to the HMOs using a risk-adjusted capitation formula.
The HMOs compete for members by offering supplementary insurance packages and operating their own local clinics. While the system is highly efficient and has excellent electronic records, it faces physician and nurse shortages, particularly in peripheral regions. The public clinics are overcrowded, leading to long wait times and a growing reliance on private specialist consultations paid for out-of-pocket or through private commercial insurance.
17. Hong Kong: Extreme Dual-Track System
Hong Kong operates a stark dual-track system: a heavily subsidized public sector (which handles ninety percent of inpatient bed-days for minimal fees) and a completely private sector (which handles outpatient care and high-end services).
The public wards are severely overloaded, with patients waiting in corridors during flu seasons and waiting years for routine joint replacements. The private sector is highly efficient and offers state- of-the-art care, but is prohibitively expensive for the average citizen. This dual track creates a class division where the poor are rationed by extreme delay, while the wealthy purchase rapid care in private hospitals.
18. Chile: The Public-Private Choice
Chile operates a dual public-private system where workers must contribute seven percent of their income to either the public national health fund (FONASA) or a private health insurance institution (ISAPRE).
The ISAPREs offer high-quality care in private clinics, but they are expensive, charge age-adjusted risk premiums, and exclude sick, high-risk patients. FONASA acts as the public safety net but is chronically underfunded, leading to long wait lists and low-quality infrastructure in public hospitals. The system is a source of intense political debate, as reformers demand the abolition of the private option to create a single-payer system, ignoring the reality that this would collapse the public sector under the weight of millions of new patients.
19. Brazil: Universal Mandate vs. Underfunded Reality
Brazil's 1988 constitution declared health as a right of all and a duty of the State, establishing the Unified Health System (SUS) to provide free, universal care to every resident.
The reality has failed the constitutional mandate. The SUS is severely underfunded, plagued by corruption, and suffers from shortages of basic medicines, long lines, and broken equipment in public clinics. Anyone who can afford it (nearly twenty-five percent of the population, including the entire middle class) purchases private health plans to bypass the public system. The SUS effectively operates as a poor-quality safety net, proving that a constitutional right to healthcare cannot generate real resources if the state cannot fund them without economic collapse.
20. India: Out-of-Pocket Dominance and Low-Cost Innovation
India has a nominal public healthcare system, but it is underfunded and of low quality. As a result, nearly seventy percent of healthcare spending in India is paid out-of-pocket directly by patients to private providers.
Because India is a direct-cash market with minimal government regulation or insurance mediation, it is highly price-sensitive. This environment has spawned world-class, low-cost private medical innovations. Hospitals like Narayana Health, founded by Dr. Devi Shetty, perform open-heart surgeries for a fraction of the cost of Western hospitals by applying assembly-line efficiency and running high-volume diagnostic centers. Private clinics compete fiercely on price and quality, making basic care highly affordable to ordinary citizens, demonstrating the power of unregulated markets to drive down costs.
The Ideal Free-Market Compromise: Price, Quality, and Safety Nets
Based on the global evidence, the path to a sustainable, high-quality healthcare system lies in re-establishing market coordination while acknowledging the political requirement for a basic safety net. An ideal free-market framework consists of four main pillars.

1. Price Transparency and Direct Payment
We must restore price signals to routine medical care. All providers: clinics, imaging centers, hospitals: should be legally required to publish clear, cash-price menus for their services online, similar to the practice in veterinary medicine or auto repair.
Routine medical transactions (annual physicals, stitches, antibiotics, x-rays) should be paid for directly by consumers out of pocket or through tax-free Health Savings Accounts (HSAs). By removing the insurance middleman from routine care, we eliminate the administrative overhead (which consumes up to thirty percent of US medical spending) and force providers to compete on price, driving costs down rapidly.
2. Direct Primary Care (DPC)
Direct Primary Care is a growing free-market business model where patients pay a flat monthly membership fee (typically fifty to one hundred dollars) directly to their primary care physician. This fee covers unlimited office visits, basic diagnostic tests, and direct access to the doctor via phone or email.
Because the doctor does not accept insurance, they do not need to hire billing staff or comply with insurance documentation requirements. This reduces their overhead by half, allowing them to manage smaller patient panels and spend more time with each patient. DPC establishes a direct, voluntary relationship between doctor and patient, returning primary care to a affordable, consumer-oriented model.
3. Catastrophic-Only Insurance
Insurance should be returned to its true purpose: protecting against low-probability, high-cost, unforeseen events. Under a free-market system, health insurance plans would be high-deductible, catastrophic policies that cover major surgeries, cancer treatments, and severe accidents.
These plans would be priced based on actual risk and decouple from employment, allowing individuals to own their policies and carry them from job to job. Premium costs would be low because the plans would not cover routine, predictable care, and consumers would have incentives to stay healthy and shop around for the best prices.
4. Competing Licensing and Supply-Side Deregulation
To lower costs, we must expand the supply of care. This requires ending the state's monopoly on medical licensing and hospital construction.
Occupational licensing should be replaced by competing private certification bodies. A doctor could be certified by the AMA, a university network, or a private quality-assurance firm, leaving consumers to decide which certification they trust. Scope-of-practice restrictions should be abolished, allowing nurse practitioners and physician assistants to operate independent clinics. Certificate of Need laws must be repealed, allowing new clinics and imaging centers to be built wherever there is market demand.
The Transition: Political Reality and Voluntary Alternatives
Implementing a complete free-market overhaul of healthcare faces immense political resistance. Special interest groups (insurance cartels, hospital lobbies, pharmaceutical companies) spend billions on lobbying to protect their government-granted monopolies. Furthermore, a public accustomed to third-party payments is fearful of paying directly for care.
To transition toward a free market, we must adopt a two-pronged strategy: political rollbacks of existing interventions and the growth of voluntary, market-based alternatives outside the state system.
Practical Political Rollbacks
To transition incrementally, we should advocate for several key reforms:
1. **Tax parity**: Allow individuals to deduct health expenses and purchase private insurance
using tax-free income, matching the tax exemption currently granted to employer-provided plans.
2. **HSA expansion**: Expand Health Savings Accounts to allow all citizens to use tax-free funds for
any medical service, including Direct Primary Care memberships and direct cash payments, removing the
requirement that they be tied to high-deductible health plans.
3. **Allow foreign drug imports**: Legalize the importation of pharmaceuticals and medical devices
approved by other developed nations, breaking the FDA's domestic monopoly.
4. **Repeal CON laws**: Strip states of the power to restrict hospital expansion and clinic
construction.
Voluntary Alternatives: Building Parallel Systems
While we lobby for political reforms, we can build parallel, voluntary institutions that operate outside the state-regulated system today.
One historical alternative is the mutual aid society. In the nineteenth and early twentieth centuries, fraternal lodges and mutual aid societies provided high-quality, affordable healthcare to millions of working-class families. Members paid small annual dues, and the lodge hired a doctor on a flat annual salary to provide unlimited care to its members. These lodge practice systems were highly efficient and affordable, until the AMA successfully lobbied the government to restrict them to protect the high fees of independent doctors. Reviving mutual aid networks and community-based health pools is a viable path to providing care without state involvement.
Another modern alternative is the Health Sharing Ministry. These are voluntary, member-based networks where participants share a common ethical framework and pool their monthly contributions to pay each other's medical bills. While they are not formal insurance plans (meaning they are exempt from state insurance regulations and mandates), they provide a highly effective, low-cost safety net for hundreds of thousands of families, operating entirely on trust and voluntary coordination.
Finally, medical tourism allows consumers to bypass domestic price distortions by traveling abroad. Countries like India, Mexico, and Costa Rica offer world-class surgeries and treatments for a fraction of the cost in the United States, operating as a direct-cash market that keeps healthcare affordable and accessible.
Conclusion: The Compassionate Market
Healthcare is too important to be left to the state. The past century of government management has proved that when we replace price signals with bureaucratic mandates, we get soaring costs, restricted supply, rationing by delay, and political corruption.
A free market in healthcare is not a system of cold indifference. It is the most compassionate system possible. By aligning the incentives of doctors and patients, encouraging price competition, and removing the state-granted monopolies that restrict supply, the market drives down costs and makes quality care affordable to everyone. By supporting Direct Primary Care, expanding Health Savings Accounts, reviving mutual aid networks, and rolling back regulatory barriers, we can take practical steps to escape the state-managed healthcare trap and build a system based on voluntary exchange, consumer choice, and genuine community care.